

.
Q. Was it a mistake to quarantine the passengers aboard the Diamond Princess in Japan?
A. The original statement, which is not unreasonable, was that the best thing to do with these people was to keep them safely quarantined in an infection-control manner on the ship. As it turned out, that was very ineffective in preventing spread on the ship. So the quarantine process failed. I mean, I’d like to sugarcoat it and try to be diplomatic about it, but it failed. I mean, there were people getting infected on that ship. So something went awry in the process of quarantining on that ship. I don’t know what it was, but a lot of people got infected on that ship. (Dr. A Fauci, Feb 17, 2020)
This is part of an interview of Dr. Anthony Fauci, the coronavirus point person we’ve been seeing so much of lately. Fauci has been the director of the National Institute of Allergy and Infectious Diseases since all the way back to 1984! You might find his surprise surprising. Even before getting our recent cram course on coronavirus transmission, tales of cruises being hit with viral outbreaks are familiar enough. The horror stories from passengers on the floating petri dish were well known by this Feb 17 interview. Even if everything had gone as planned, the quarantine was really only for the (approximately 3700) passengers because the 1000 or so crew members still had to run the ship, as well as cook and deliver food to the passenger’s cabins. Moreover, the ventilation systems on cruise ships can’t filter out particles smaller than 5000 or 1000 nanometers.[1]
“If the coronavirus is about the same size as SARS [severe acute respiratory syndrome], which is 120 nanometers in diameter, then the air conditioning system would be carrying the virus to every cabin,” according to Purdue researcher, Qingyan Chen, who specializes in how air particles spread in different passenger crafts. (His estimate was correct: the coronavirus is 120 nanometers.) Halfway through the quarantine, after passenger complaints, they began circulating only fresh air–which would have been preferable from the start. By then, however, it is too late: the ventilation system is already likely filled with the virus, says Chen.[2] Arthur Caplan, the bioethicist who is famous for issuing rulings on such matters, declares that
“Boats are notorious places for being incubators for viruses. It’s only morally justified to keep people on the boat if there are no other options.”
Admittedly, it is hard to see an alternative option to accommodate so many passengers for a 2 week quarantine on land, and there was the possible danger of any infections spreading to the local population in Japan. So, by his assessment, it may be considered morally justified.
The upshot: As of 19 March 2020, at least 712 out of the 3,711 passengers and crew had tested positive for covid-19; 9 of those who were on board have died from the disease (all over the age of 70). As I was writing this, I noted a new CDC report on the Diamond Princess as well as other cruise ships; they state 9 deaths.[3] A table on the distribution of ages of passengers on the Diamond Princess is in Note [4].
So how did the Diamond Princess cruise ship become a floating petri dish for the coronavirus from Feb 4-Feb 20?
The Quarantine
It was their last night of a 2-week luxury cruise aboard the Diamond Princess in Japan (Feb 3) when the captain came on the intercom. He announced: a passenger on this ship who disembarked in Hong Kong 9 days ago (Jan 25) has tested positive for the coronovirus. (He was on board for 5 days.) Everyone will have to stay on board an extra day to be examined by the Japanese health authorities. A new slate of activities was arranged to occupy passengers during the day of health screening–later mostly dropped. But on the evening of February 3, things continued on the ship more or less as before the intercom message.
“The response aboard the Diamond Princess reflected concern, but not a major one. The buffets remained open as usual. Onboard celebrations, opera performances and goodbye parties continued”. (NYT, March 8)
The next day, as health officials went door to door to screen passengers, guests still circulated on board, lined up for buffets, and used communal spaces. But then, the following morning (Feb 5), as guests were heading to breakfast, the captain came over the intercom again. He announced that 10 people had tested positive for the coronavirus and would be taken off the ship. Everyone else would now have to be quarantined in their cabins for 14 days. The second day of the quarantine (Feb 6) it was announced that 20 people more had tested positive, then on day three, 41 more, then 64 more, and on and on. By the end of the quarantine on February 19 at least 621 on the ship had tested positive for the virus.
Adding to the stress, “we quickly learned that our tests were part of an initial batch of 273 samples and that the first 10 cases reported on day one were only from the first 31 samples that had been processed” from the passengers with highest risk. (U.S. passenger, Spencer Fehrenbacher, interviewed on the ship)
As the number of infected ballooned, passengers were not always informed right away; some took to counting ambulances lined up outside to find out how many new cases would be announced at some point. I wonder if the passengers were told that the very first person to test positive was a crew member responsible for preparing food. In fact, by February 9, around 20 of the crew members tested positive, 15 of which were workers preparing food. Crew members lived in close quarters, shared rooms and continued to eat their meals together buffet-style. They had no choice but to keep running the ship as best as they could.
“Feverish passengers were left in their rooms for days without being tested for the virus. Health officials and even some medical professionals worked on board without full protective gear. [Several got infected.] Sick crew members slept in cabins with roommates who continued their duties across the ship, undercutting the quarantine”. (NYT Feb 22)
Passengers in cabins without windows (and later, others) were allowed to walk on deck, six feet apart, for a short time daily. Unfortunately, presumed infection-free “green zones” were not rigidly separated from potentially contaminated “red zones”, and people walked back and forth between them. Gay Courter, a writer from the U.S. who, as it happens, situated one of her murder mysteries on a cruise ship, told Time “It feels like I’m in a bad movie. I tell myself, ‘Wake up, wake up, this isn’t really happening.’” (Time, Feb 11). This is the same bad movie we are all in now, except our horror tale has gotten much worse than on Feb 10.
At some point, I think Feb 10, the ship became the largest concentration of Covid-19 cases outside China, which is why you’ll notice the Diamond Princess has own category in the data compiled by the World Health Organization (Worldometer).
In a Science Today article, a Japanese infectious disease specialist regretted the patchwork way in which passenger testing was done:
Japan has missed a chance to answer important epidemiological questions about the new virus and the illness it causes. For instance, a rigorous investigation that tested all passengers at the start of the quarantine and followed them through to the end could have provided information on when infections occurred and answered questions about transmission, the course of the illness, and the behavior of the virus.
(They were only able to test people in stages.) A similar paucity of testing in the U.S. robs us from crucial information for understanding and controlling the coronavirus. However, there is a fair amount being gleaned from the Diamond Princess, as you can see in the references below. (Please share additional references in the comments.) More is bound to follow.
Estimates from the Diamond Princess
“Data from the Diamond Princess cruise ship outbreak provides a unique snapshot of the true mortality and symptomatology of the disease, given that everyone on board was tested, regardless of symptoms”–or at least virtually all. [link] The estimates (from the Diamond Princess) I’ve seen are based on those from the London School of Hygiene and Tropical Medicine, in a paper still in preprint form,”Estimating the infection and case fatality ratio for COVID-19 using age-adjusted data from the outbreak on the Diamond Princess cruise ship”.
Adjusting for delay from confirmation-to-death, we estimated case and infection fatality ratios (CFR, IFR) for COVID-19 on the Diamond Princess ship as 2.3% (0.75%-5.3%) [among symptomatic] and 1.2% (0.38-2.7%) [all cases]. Comparing deaths onboard with expected deaths based on naive CFR estimates using China data, we estimate IFR and CFR in China to be 0.5% (95% CI: 0.2-1.2%) and 1.1% (95% CI: 0.3-2.4%) respectively. (PDF)
(For definitions and computations, see the article.) These are lower than the numbers we are often hearing. They used their lower fatality estimates to adjust (down) the estimates from China data. The paper lists a number of caveats.[5] I hope readers will have a look at it (it’s just a few pages) and share their thoughts in the comments. (Their estimates are in sync with an article by Fauci et al., to come out this week in NEJM; but whatever the numbers turn out to be, we know our healthcare system, in many places, is being overloaded. [6])
Another study takes the daily reports of infections on the Diamond Princes to attempt to evaluate the impact of the quarantine, as imperfect as it was, in comparison to a counterfactual situation where nothing was done, including not removing infected people from the ship. They estimate nearly 80%, rather than 17% would have been infected. [link]
We found that the reproductive number [R0] of COVID-19 in the cruise ship situation of 3,700 persons confined to a limited space was around 4 times higher than in the epicenter in Wuhan, where was estimated to have a mean of 3.7.[7]
The interventions that included the removal of all persons with confirmed COVID-19 disease combined with the quarantine of all passengers substantially reduced the anticipated number of new COVID-19 cases compared to a scenario without any interventions (17% attack rate with intervention versus 79% without intervention) … However, the main conclusion from our modelling is that evacuating all passengers and crew early on in the outbreak would have prevented many more passengers and crew members from getting infected.” [link]
Only 76, rather than 621 would have been infected, they estimate. [8]
Conclusions: The cruise ship conditions clearly amplified an already highly transmissible disease. The public health measures prevented more than 2000 additional cases compared to no interventions. However, evacuating all passengers and crew early on in the outbreak would have prevented many more passengers and crew from infection.
These studies and models are of interest, although I’m in no position to evaluate them. Please share your thoughts and information, and point out any errors you find. I will indicate updates in the title of this post.
Optimism
I leave off with the remark of one of the U.S. passengers interviewed while still on the Diamond Princess:
“Being knee deep in the middle of a crisis leaves a person with two options — optimism or pessimism. The former gives a person strength, and the latter gives rise to fear.” (link)
He, like the others who were evacuated, faced an additional 2 weeks of quarantine.[9] He has since returned home and remains infection free.
*****
[1] As a noteworthy aside, Fauci was able to assure the interviewer that the “danger of getting coronavirus now is just minusculely low” (in the U.S. on Feb. 17). What a difference 2 weeks can make.
[2] In a 2015 paper, Chen and colleagues found a cruise ship’s ventilation spread particles from cabin to cabin. They found that 1 infected person typically led to more than 40 cases a week later on a 2000 passenger cruise. By contrast, the coronavirus, with a reproductive rate of 2 cases per infected person, would only lead to 3 new cases during that time. Planes rely on high-strength air filters and are designed to circulate air within cabin sections.
[3] In a March 23 CDC report: Among 3,711 Diamond Princess passengers and crew, 712 (19.2%) had positive test results for SARS-CoV-2. Of these, 331 (46.5%) were asymptomatic at the time of testing. Among 381 symptomatic patients, 37 (9.7%) required intensive care, and nine (1.3%) died (8).
They found coronavirus in Diamond Princess cabins 17 days after passengers disembarked (prior to cleaning).
[4] A table from the Japanese National Institute of Infectious Diseases (NIID) (Source LINK):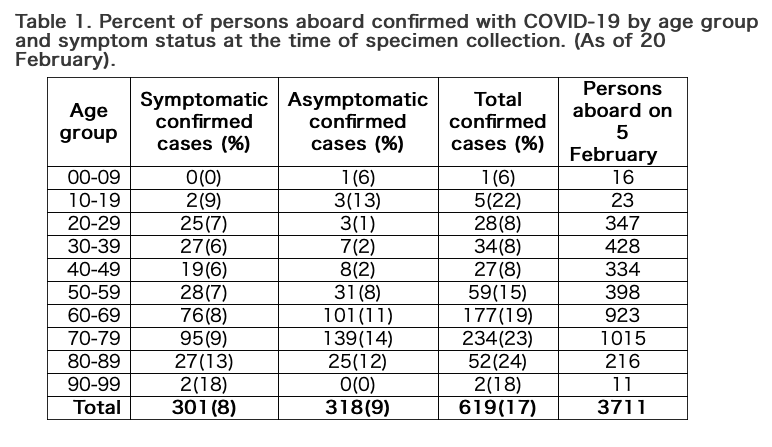
[5]
“There were some limitations to our analysis. Cruise ship passengers may have a different health status to the general population of their home countries, due to health requirements to embark on a multi-week holiday, or differences related to socio-economic status or comorbidities. Deaths only occurred in individuals 70 years or older, so we were not able to generate age-specific cCFRs; the fatality risk may also be influenced by differences in healthcare between countries”.
[6] In a March 26 article by Fauci and others, Covid-19 — Navigating the Uncharted, we read:
“If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%.”
[7] R0 may be viewed as the expected number of cases generated directly by 1 case in a susceptible population.
[8] The number in the most recent report is 712, but that would be after the quarantine ended on Feb 19.
[9] I read today that one of the U. S. evacuated passengers just entered a clinical trial on remdesivir. This would be over a month since the end of the first quarantine.
———–
REFERENCES:
- Fauci interview: ‘Danger of getting coronavirus now is just minusculely low‘
- Giwa, A., LLB, MD, MBA, FACEP, FAAEM; Desai, A., MD; Duca, A., MD; Translation by: Sabrina Paula Rodera Zorita, MD (2020). “Novel 2019 Coronavirus SARS-CoV-2 (COVID-19): An Updated Overview for Emergency Clinicians – 03-23-20” EBMedicine.net; Pub Med ID: 32207910; (LINK)
- Japanese National Institute of Infectious Diseases (NIID). “Field Briefing: Diamond Princess COVID-19 Cases, 20 Feb Update” (LINK)
- Russell, T., Hellewell, J.,Jarvis, C., van-Zandvoort, K.Abbott, S.,Ratnayake, R., Flasche, S., Eggo, R. & Kucharski, A. (2020). “Estimating the infection and case fatality ratio for COVID-19 using age-adjusted data from the outbreak on the Diamond Princess cruise ship.” MedRXIV: The preprint server for the Health Sciences. (March 9, 2020). (PDF)
- Zheng, L., Chen, Q., Xu, J., & Wu, F. (2016). Evaluation of intervention measures for respiratory disease transmission on cruise ships. Indoor and Built Environment, 25(8), 1267–1278. (First Published online August 28, 2015 ). (PDF)


")


Thanks for posting this discussion. It was enlightening.
James: Thank you so much for reading and including a comment.
Thank you for this interesting article and analysis.
It is very regrettable that we don’t know when each passenger contracted the virus. It would be helpful to know how many were infected prior to the “lockdown” and how many more contracted it (other than from their cabin mate) during that period. That would be tremendously interesting and also help quantify the concern about the recycled air and inadequate filters.
It is interesting that passengers with symptoms were matched by only one infected/asymptomatic extra case.
Another surprise is that the asymptomatic passengers didn’t skew to the younger age groups. The sample sizes are low, but it almost seems as if younger passengers may have been more likely to be symptomatic than older ones. That’s a curious contrast with the morbidity rates.
I’m also surprised by the suggested R0 rate of 3.0 in Wuhan. To be blunt and also polite, none of the Chinese data is very robust; I tried to trace the references that evidenced this claim back, but came to a dead end with a non-online reference. My sense, and I’ve not tried to model any of the data, is that the R0 “felt” like less than 3, although of course a lot depends on the serial interval as well.
But the massively greater R0 claimed for the ship really just points that a ship is not a good model to use for an “ordinary” environment. And that, at last, is really my point. That we lack adequate data to fully understand the Diamond Princess case, and that in any event, the special nature of the cruise ship environment does not translate reliably to regular populations ashore.
David:
Thank you so much for your comments. You point out a number of things I hadn’t noticed, e.g., about ages of asymptomatic cases.
“It is very regrettable that we don’t know when each passenger contracted the virus. It would be helpful to know how many were infected prior to the “lockdown” and how many more contracted it (other than from their cabin mate) during that period.”
It would be great to know this. If everyone had been tested at the start, it would have been clear, or at least clearer. The Hong Kong passenger had symptoms on Jan 22, and there was another passenger who did on Jan 23 (who also tested positive). In the “official” reports it is surmised that the majority of the infections occurred before the quarantine. That would mean during the 5 days the Hong Kong passenger was on board. I can’t help feeling that the health officials are being defensive in presuming this, since otherwise, they’d have to admit transmission occurred during the quarantine (and not just between the crew members who lived and ate together). Fauci, on the other hand, in saying the quarantine failed, is clearly saying there was transmission during the quarantine. But he claims to be mystified as to what went awry.
“But the massively greater R0 claimed for the ship really just points that a ship is not a good model to use for an “ordinary” environment. And that, at last, is really my point.”
True, but it reflects what could be the case since, after all, it really was the case on the ship. I wonder that there isn’t more discussion today of the possible spread through recirculated air. As I was reading about this, I began walking outside here more (I live in the mountains in the country), and will open windows when it’s warm enough.
I wonder if they contrasted infections among those in windowless cabins and those with outside decks. (Of course there are confounders).
I noticed in the “related posts” that WordPress automatically generates, that there was a 2014 post on Ebola, quarantines, and Arthur Caplan saying that quarantines were a bad idea (then). Here’s the link: https://errorstatistics.com/2014/10/26/to-quarantine-or-not-to-quarantine-science-policy-in-the-time-of-ebola/
ED Note: This comment refers to a different post to which I allude in my comment: https://errorstatistics.com/2014/10/26/to-quarantine-or-not-to-quarantine-science-policy-in-the-time-of-ebola/) I brought it over here so that people would find it.
Language is powerful. In the present hornets’ nest atmosphere both precision and accuracy of speech need our closest attention. Dr. Caplan is a philosopher and brilliant thinker but he is neither a physician nor public health expert. He seems confused about both the meaning and medical importance of “Quarantine”.
He betrays gross misunderstanding in his very first bullet point, “Quarantining people without symptoms makes no scientific sense”. What really makes no sense at all is Caplan’s very first sentence!
Quarantine is a public health tool used for observing people who have had a credible exposure but NO SYMPTOMS. Caplan makes a layman’s mistake in getting confused by two facts: (1) quarantine involves isolating plausibly well people from society and (2) SICK people are also isolated during their treatment/recovery. Sick people with any contagious disease absolutely must be isolated from open society during their recovery period to prevent disease spread. Deep confusion about the meaning of “quarantine” is very widespread right now — watch CNN or MSNBC for 15 minutes and you can see for yourself.
The utility of quarantine as a combined detection / prevention tool goes back many years in the history of public health and the term refers to the process of removing ASYMPTOMATIC people who have been credibly exposed from all contact with open society for a defined period of time (T) in order to observe these isolated people for reliable signs/symptoms of some disease X. Quarantine does reduce the spread of contagious diseases that are transmissible by human-to-human contact. The value of T is determined from empirical knowledge of the maximum incubation period for disease X as recorded for large numbers of past cases. Incubation period is defined as the number of days between exposure and the date of disease X development. Some exposed people develop a disease very quickly and obviously; others may not develop disease that promptly.
For COVID19, T = 14 days and the median incubation period is known to be between 5 and 6 days. The nasty skunk at the picnic here is that people who have COVID19 disease can be highly contagious virus shedders, yet feel just peachy during their early incubation period. Not all contagious diseases are like that.
In sum, if quarantined person Joe Smith does not become ill during T days of isolation from society, we can conclude with high confidence that Mr. Smith has not contracted disease X. On the other hand, if a quarantined person DOES develop findings that pin down the diagnosis of X during time T, the process of quarantine has not only allowed diagnosis of X at the earliest possible moment, but it has also prevented that person from exposing other people. Quarantine breaks the chain of transmission from persons who are asymptomatic but shedding dangerous pathogens during their incubation period.
I understand that Dr. Caplan’s “points” were made in the context of a discussion about Ebola virus infections. Nonetheless, in the present COVID19 disaster it is absolutely certain that we are dealing with a new disease that is (a) Highly contagious, and (b) Definitely transmissible from persons who are carriers of the virus even though not yet symptomatic (they look well, feel well etc.). There is one more thing to note — Ebola is much more lethal than COVID19 and the irony here (or is it a paradox?) is that COVID19 arguably is far more insidious than Ebola because COVID19 victims can “stick around” much longer while shedding active SARS-CoV-2 virus.
The lay public may be getting unwittingly hoodwinked in hearing from our government that “80 percent of you will be just fine if you get this illness”. Mr. Pence keeps sending that basic message although in not so many words. Well, yes maybe, contingent on the meaning of “just fine”. But persons who have “mild” COVID19 disease do also shed the active virus. COVID19 is a highly contagious disease that, unlike Ebola infection, does not incapacitate its victims rapidly. Quarantine is an absolutely essential tool in the present chaos.
(Comment originally posted today under: https://errorstatistics.com/2014/10/26/to-quarantine-or-not-to-quarantine-science-policy-in-the-time-of-ebola/)
James: I moved the comment you made on my 2014 post, mentioning Caplan) to this post since it is relevant, and no one would find it there. I doubt Caplan feels that way about today’s quarantines. On the “paradox”, I think that’s precisely what we expect from natural selection, too lethal and you kill all your hosts.
I’d be interested to hear more of what you think regarding today’s covid-19 policies.
A tweet by Ron Kenett:
This link says 10 deaths, but the CDC report says 9. This is 2 months out of course.
https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html
Mayo is handling this as an applied statistician would. We are facing an unstructured problem. The first step in the life cycle view is to do some problem elicitation so that is can be handled in an analytic space. She then considers all dimensions of information quality. Given data, X, goal, g, analysis methods, f and utility, U, the InfoQ she generates has high: InfoQ=U[f(X\g)}.
The three points worth expanding on are: 6) Generalisation of findings, 7) Operationalisation of findings and 8) Communication of findings.
i) How can the Princess cruise data analysis findings be applied to other situations
ii) How can these findings turn into policy decisions
iii) How can this interesting analysis be communicated to the right persons at the right time.
Stronger responses to these would make the information quality in Mayo’s blog even stronger.
The corona virus global crisis is also a crisis of information quality. There seems to be a herd effect in policies implemented by governments. The aggregated data we get in more and more fancy graphs do not account for local effects. We are information poor, and this carries a terrible price.
For more on reviewing applied work with information qualty dimensions see 10.3233/SJI-160967
For the evolution of quality, from product quality to information quality see https://www.linkedin.com/pulse/evolution-quality-from-product-information-ron-s-kenett/
For a life ccycle view of statistcis see http://andrewgelman.com/wp-content/uploads/2017/08/Kenett-Life-Cycle-QE-2015.pdf
For a ten questions on statistics and data science see https://www.linkedin.com/pulse/ten-questions-statistics-data-science-2020-beyond-ron-s-kenett/
Ron: Thanks for your comment. I had pasted your tweet on this earlier. I really don’t see my post as akin to applied statistics. I’m just telling a story, emphasizing philosophical assumptions/puzzles in order to make a few points that seem in need of attention: the need to be testing for covid-19 much more prevalently in the U.S.(info we missed from the limited testing on the DP), the relevance of the stats from the ship (given the avenues for transmission), and the possibility of spread through some kinds of ventilation systems. Finally, a last word to try and cheer myself, and readers, up.
I thought you would want to distance yourself from applied statistics…:-)
In many cases, the story telling part as you did, is the essential part in an applied statistics report.
I assume the story you tell about the Corona Princess, is meant to convey information.
As a philosopher of science, how would you assess/discuss/present the information quality of your story??
My answer is structured on the basis of the information quality framework I presented many times. Based on such an assessment I found your Corona Princess blog of high information quality.
Ron:
In your assessment, it’s not clear how you’d distinguish applied stat from science journalism. I intended more than the latter, but something “less” than the former. But I thank you for saying it’s of “high quality”!
Nature.com has a 3/26 article that contains a lower estimate of the IFR, which is encouraging:
By contrast, Russell and his colleagues used data from the ship — where almost everyone was tested, and all seven deaths recorded — and combined it with more than 72,000 confirmed cases in China, making their CFR estimate more robust. The results have been posted on the biomedical preprint server medRxiv, and have not been peer-reviewed yet.
The group also estimates that the infection fatality rate (IFR) in China — the proportion of all infections, including asymptomatic ones, that result in death — is even lower, at roughly 0.5%. The IFR is especially tricky to calculate in the population, because some deaths go undetected if the person didn’t show symptoms or get tested.
Here is the link: https://www.nature.com/articles/d41586-020-00885-w
William:
Thank you so much for your comment and for the link to the Nature article; they’re both very helpful. Do you have any thoughts as to why there appear to be so many asymptomatic cases? As an earlier commentator noticed, surprisingly, asymptomatics were more prevalent in older than younger groups, although, admittedly, the number of infected in the latter are small. But why, in general, are there asymptomatics. The Chinese did not count asymptomatics in their data on confirmed cases.
I’m glad the mortality estimates being given seem to be coming down. I know it’s taboo to compare the mortality of covid-19 and ordinary flu (Fauci gives the former as 10 times as deadly as the latter, which may be right)–since whatever the numbers are, we know we have a dangerously overloaded healthcare system– but I’m struck by the CDC report on flu for Oct 1-March 21 for the U.S.:
CDC estimates for the U.S.: from October 1, 2019, through March 21, 2020, there have been 38,000,000 – 54,000,000 flu illnesses, 18,000,000 – 26,000,000 flu medical visits, 400,000 – 730,000 flu hospitalizations, 24,000 – 62,000 flu deaths
https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm
I realize the hospitalizations for flu are only a few days (unlike with covid-19, which are longer), and we don’t see kind of need for ventilators as with covid-19–and these differences are crucial for the issue of hospital overload– but they are still saying more than 23,000 deaths in ~23 weeks.
Another reference on DP stats:
Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020
https://eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.10.2000180
Most respiratory viral infections cause asymptomatic infections in some people:
Galanti M et al (2019). Rates of asymptomatic respiratory virus infection across age groups. Epidemiology and Infection 147, e176, 1–6. doi.org/10.1017/ S0950268819000505
Abstract
Respiratory viral infections are a leading cause of disease worldwide. A variety of respiratory viruses produce infections in humans with effects ranging from asymptomatic to life-treath- ening. Standard surveillance systems typically only target severe infections (ED outpatients, hospitalisations, deaths) and fail to track asymptomatic or mild infections. Here we performed a large-scale community study across multiple age groups to assess the pathogenicity of 18 respiratory viruses. We enrolled 214 individuals at multiple New York City locations and tested weekly for respiratory viral pathogens, irrespective of symptom status, from fall 2016 to spring 2018. We combined these test results with participant-provided daily records of cold and flu symptoms and used this information to characterise symptom severity by virus and age category. Asymptomatic infection rates exceeded 70% for most viruses, excepting influenza and human metapneumovirus, which produced significantly more severe outcomes. Symptoms were negatively associated with infection frequency, with children displaying the lowest score among age groups. Upper respiratory manifestations were most common for all viruses, whereas systemic effects were less typical. These findings indicate a high burden of asymptomatic respiratory virus infection exists in the general population.
Two possible reasons for this include variations in immune systems of people and variations in the number of viral particles to which different people are exposed.
Here’s a link of an interview with a well-known person in virology, David Offit. In this interview March 19, he still thinks we are over-reacting. Try this:
https://www.physiciansweekly.com/covid-19-is-our-cure-worse-than-the-disease-with-dr-paul-offit/
That link to Offit interview is leading me to a 404 Error, says not available etc. What did I do wrong?
Sorry, try the one I replaced it with.
I watched that entire video this morning. A very important scientist and a well-done interview that covers many key sub-topics in the COVID19 matter. Thanks so much for putting this link up on your site. Hope you are doing well Deborah.
James: Thank you, I liked it too. I found an even more recent interview of him. He still seems to think there’s an overreaction, and thinks that the panic is making things worse. Do you agree with him? He was one of the people to create a vaccine for (I believe it’s) the rotovirus.
I’m doing OK so far. Hope you are as we.
This article in a premier gastroenterology journal, Gastroenterology, supports Dr. Offit’s opinion of enteric spread of coronavirus by showing that the related SARS virus does spread by the fecal-oral route.
Enteric involvement of severe acute respiratory syndrome-associated coronavirus infection1
Wai K Leung∗, Ka-fai To‡, Paul K.S Chan§, Henry L.Y Chan∗, Alan K.L Wu∗, Nelson Lee∗, Kwok Y Yuen∥, Joseph J.Y Sung∗
PlumX Metrics
DOI: https://doi.org/10.1016/j.gastro.2003.08.001
Abstract
Full Text
Images
References
Abstract
Math Eq: Severe acute respiratory syndrome (SARS) is a recently emerged infection from a novel coronavirus (CoV). Apart from fever and respiratory complications, gastrointestinal symptoms are frequently observed in patients with SARS but the significance remains undetermined. Herein, we describe the clinical, pathologic, and virologic features of the intestinal involvement of this new viral infection. Math Eq: A retrospective analysis of the gastrointestinal symptoms and other clinical parameters of the first 138 patients with confirmed SARS admitted for a major outbreak in Hong Kong in March 2003 was performed. Intestinal specimens were obtained by colonoscopy or postmortem examination to detect the presence of coronavirus by electron microscopy, virus culture, and reverse-transcription polymerase chain reaction. Math Eq: Among these 138 patients with SARS, 28 (20.3%) presented with watery diarrhea and up to 38.4% of patients had symptoms of diarrhea during the course of illness. Diarrhea was more frequently observed during the first week of illness. The mean number of days with diarrhea was 3.7 ± 2.7, and most diarrhea was self-limiting. Intestinal biopsy specimens obtained by colonoscopy or autopsy showed minimal architectural disruption but the presence of active viral replication within both the small and large intestine. Coronavirus was also isolated by culture from these specimens, and SARS-CoV RNA can be detected in the stool of patients for more than 10 weeks after symptom onset. Math Eq: Diarrhea is a common presenting symptom of SARS. The intestinal tropism of the SARS-CoV has major implications on clinical presentation and viral transmission.
Exponential growth in disease epidemics is shocking. Most people really don’t understand exponential growth well at all. For example, if the number of cases is doubling every 6 days (a slower rate for this virus) and somebody notes “oh, our hospitals are only half full”, well they will be full in 6 days. Exponential growth trickles along at an apparently low, linear rate in early phases, then absolutely rockets skyward. People are lulled during that initial phase, then stunned when the rocketing happens.
The Offit interview occurred on March 17. We can re-evaluate it in a couple of months, or years. I predict it will not hold up well.
Fecal-oral: Offit goes on at length about fecal-oral transmission, yet there is no evidence yet to support this route of transmission.
WHO:
Click to access who-china-joint-mission-on-covid-19-final-report.pdf
the fecal-oral route does not appear to be a driver of COVID-19 transmission; its role and significance for COVID-19 remains to be determined.
CDC (USA)
https://www.cdc.gov/coronavirus/2019-ncov/php/water.html
Is the COVID-19 virus found in feces?
The virus that causes COVID-19 has been detected in the feces of some patients diagnosed with COVID-19. The amount of virus released from the body (shed) in stool, how long the virus is shed, and whether the virus in stool is infectious are not known.
The risk of transmission of COVID-19 from the feces of an infected person is also unknown. However, the risk is expected to be low based on data from previous outbreaks of related coronaviruses, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS). There have been no reports of fecal-oral transmission of COVID-19 to date.
Public Health Ontario (Canada)
https://www.publichealthontario.ca/-/media/documents/ncov/what-we-know-feb-06-2020.pdf?la=en
Respiratory droplets are likely the predominant mode of transmission for the 2019-nCoV. The extent to which fecal-oral transmission contributes to the spread of 2019-nCoV is not yet known.
At minute 14:30 Offit quotes an Indian researcher who says in regard to the rotovirus: “If everyone is infected in many areas regardless of levels of sanitation then it must be a respiratory transmission.”
Well that is precisely what we are seeing here. This disease is running rampant everywhere. That does not happen by fecal-oral transmission in this day and age of water sanitation. So all the discussion of fecal-oral is a big distraction here.
Economic demise:
What is the damage that will occur by adopting sheltering behaviours to save lives? How many lives will be lost from an economic slowdown?
Minute 18:50: Offit: “Most people live paycheck to paycheck”. The fallout from this sad episode will show that running a society where most people live paycheck to paycheck puts them at far greater risk of illness and death. This is a cultural choice Americans have made, and these are the consequences. An alternative is to stop this paycheck to paycheck nonsense. Andrew Yang is right, if you give people a basic income, they will be able to weather setbacks such as this. This will of course be endlessly debated for years to come, but the severity of impact of this virus will be greater in countries where many people have little means to support themselves and their health.
Americans often tout that America is the richest nation on earth, and there’s plenty of data over decades to support such a stance. But who has that wealth?
Are we really at the point where we tell 2 million Americans that it is time to die to save the economy and prop up the wealth of a handful of rich people? Which 2 million shall die? When is the last time we had nearly 1% of our population die within a few months?
From the Guardian: Prof Sarath Ranganathan, a board member of Lung Foundation Australia and director of respiratory and sleep medicine at Melbourne’s The Royal Children’s Hospital, said: “The experience in Italy and Spain, and the modelling used by mathematicians around the world, indicates the number of people who will become critically ill with Covid-19 will greatly exceed the capacity to care for them using respiratory support.
“Without access to ventilators many patients who might survive the infection will die.”
How many? If ventilators are not doing anything, why do we need them? I can’t find any good data right now, but is there really this much clamor for ventilators if they do nothing?
What proportion of the population will get infected when we all go back to work? When does herd immunity kick in? 50% infected? 80% infected?
So the death rate will be closer to 10% than 1% when we order all Americans back to work and 150-240 million people get sick. There will not be enough ventilators for so many people, and the death rate will leave many more than 2 million dead. What kind of a society will we be left with, after 5-10% of our paycheck to paycheck citizens have been culled? Which 5-10% of business leaders shall we deny medical care, and what will the state of our economy be after their demise?
We can print money and send it to the paycheck to paycheck people, keep a minimal wartime-like economy going (plenty of home industry available right now, making masks, running 3D printers for face shields, on and on), and avoid becoming a savage devil-take-the-hindmost culture.
I will not be looking to Dr. Offit for clarity of guidance during this pandemic.
Steven:
So great to get your comment, chock full of interesting thoughts and links. Before I study them fully, I just wanted to raise a few points/queries:
It’s interesting what you say about likely mode of transmission. What do you think the major route was on the Diamond Princess?
If the major transmission route is respiratory, shouldn’t we be seeing a marked decrease in ordinary flu? I don’t know if we are, the CDC numbers are high.
If you think Offit is underreacting, I wonder what you think of Ioannidis: https://www.stress.org/stanford-professor-data-indicates-were-severely-overreacting-to-coronavirus
That this is from just a few days ago, linking to his March 17 piece, suggests he still holds this view. He’s right, I think, to worry about consequences, not just economic, but utter social breakdowns–let’s hope not, but prisoners are being released, and it’s not far-fetched for people to need to protect themselves. And what about the extra deaths from operations being put on hold?
You’re very critical of the U.S. I’d very much like to know what you would recommend? Are we doing the right thing at this point? Is Canada (which has a much lower incidence)?
Today’s sad news pretty much obliterates Ioannidis’ March 17 opinion about seeing only 10,000 deaths in the USA.
https://www.washingtonpost.com/world/2020/04/06/coronavirus-latest-news/
Live updates: Surgeon general warns of ‘hardest, saddest week’ ahead as U.S. coronavirus deaths surpass 10,000
April 6, 2020 at 12:07 p.m. PDT
Steven:
No one knows where Ioannidis got that number from.
The current CDC estimates of regular flu are:
CDC estimates that, from October 1, 2019, through March 28, 2020, there have been:
39,000,000 – 55,000,000 flu illnesses, 18,000,000 – 26,000,000
flu medical visits, 400,000 – 730,000 flu hospitalizations, 24,000 – 63,000 flu deaths
https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm
One would think that in estimating covid-19 deaths, mortality in ordinary flu would be a minimal projection,and Ioannidis’ numbers are lower.
Returning to covid-19 deaths, you were correct in your April 2 prediction that we’d be at 10,000 today.
I have no idea why that comment didn’t go through, I do now know why your comment was held, it’s the number of links. I don’t know why I wasn’t alerted though. I am changing the settings to avoid that happening again.At least we didn’t set a new record for yesterday, we’ll see how today goes. Given how backed up testing is, it’s hard to assess these numbers.
Ioannidis states in his STAT article:
“In the absence of data, prepare-for-the-worst reasoning leads to extreme measures of social distancing and lockdowns. Unfortunately, we do not know if these measures work.”
linking to a Cochrane review article
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD006207.pub4/epdf/full
which includes conclusions such as “There was limited evidence that social distancing was effective, especially if related to the risk of exposure.”, “There is insufficient evidence to support screening at entry ports and social distancing (spatial separation of at least one metre between those infected and those non-infected) as a method to reduce spread during epidemics.”
Meanwhile, areas that have implemented social isolation and distancing continue to show improvement in slowing infection rates, while those that do not show tragic exponential growth.
We also do not have any evidence that eye glasses work. Just try to find randomized clinical trials to ascertain whether eye glasses do anything as compared to no glasses.
Some things are so obvious that we just get on with them without scheduling randomized clinical trials. Giving eye glasses to a struggling school child frequently results in such obvious improvements in performance that a high-quality evidence study is simply not necessary, and would probably not pass ethical muster in many locales.
Hundreds of years of quarantining activity cannot all have been for naught. Isaac Newton was not wrong to hole up in his country lodgings while the plague ripped through London. Lack of Cochrane Review evidence of this or that quality is not proof that distancing does nothing. Of course these measures work.
Steven:
When my eye doctor has me run through 10 or 20 potential combinations for glasses, I pick the one that best gets rid of blurriness, it has nothing to do with a statistical effect that would call for a randomized test procedure. That said, I’m not questioning that quarantines work to curb transmissible diseases.
I have to read and listen to Dr. Anthony Fauci’s statements quite carefully now, I’m unclear on what strategy he is gaming out these days. I tip my hat for his years of public service at NIAID, but I have to wonder how much in the loop he is.
Why did Fauci say on February 17, 2020, “We only have 15 cases in the United States, 13 of which are travel, two of which are spouses of the travelers. As of Monday morning, we now have 14 additional ones, because we flew in the people from the (Diamond Princess) cruise ship.” (USA Today article https://www.usatoday.com/story/opinion/2020/02/17/new-coronavirus-what-dont-we-know-dr-anthony-fauci-q-a-opinion/4790996002/ hyperlinked above)
How much testing had been done, or not done, in the USA by mid-February?
https://www.washingtonpost.com/politics/2020/03/30/11-100000-what-went-wrong-with-coronavirus-testing-us/
“By Feb. 16, the CDC and state public health labs tested nearly 1,600 specimens. As a rule of thumb, two specimens are required per person, meaning that in total, only about 800 people had been tested. That’s roughly 2.4 tests per million people in the United States. In contrast, South Korea, which found its first case on the same day as the United States, had tested nearly 8,000 people, or 154.7 tests per million.”
Did Anthony Fauci know this? If he didn’t, why am I listening to him? If he did, why would he say “we only have 15 cases”? An honest scientist would say “We have 15 known cases, but with very little testing and contact tracing, we really don’t know how many other cases are in America”. Fauci’s stature and the confidence with which he makes such statements is not helping us here.
Now China had its early episode of a doctor sounding the alarm, only to be hushed by authorities.
https://www.theguardian.com/world/2020/feb/06/whistleblower-chinese-doctor-dies-from-coronavirus
“A whistleblowing Chinese doctor who tried to raise the alarm about the coronavirus outbreak has died, a Communist party-controlled newspaper has confirmed.
Li Wenliang, 34, was declared dead at 2.58am local time on Friday morning after ’emergency treatment’ at a hospital in Wuhan, the Global Times reported, following hours of confusion over his fate.”
Young people are dying from coronavirus infections, and this is a tragic example.
Meanwhile in Seattle,
“Dr. Helen Y. Chu, an infectious disease expert in Seattle, knew that the United States did not have much time.
In late January, the first confirmed American case of the coronavirus had landed in her area. Critical questions needed answers: Had the man infected anyone else? Was the deadly virus already lurking in other communities and spreading?
As luck would have it, Dr. Chu had a way to monitor the region. For months, as part of a research project into the flu, she and a team of researchers had been collecting nasal swabs from residents experiencing symptoms throughout the Puget Sound region.
To repurpose the tests for monitoring the coronavirus, they would need the support of state and federal officials. But nearly everywhere Dr. Chu turned, officials repeatedly rejected the idea, interviews and emails show, even as weeks crawled by and outbreaks emerged in countries outside of China, where the infection began.
By Feb. 25, Dr. Chu and her colleagues could not bear to wait any longer. They began performing coronavirus tests, without government approval.”
For four weeks after the initial case in Seattle, US CDC and other officials sat on evidence available while an exponentially growing epidemic unfolded. Fauci claims on Feb 17 that there’s only 15 cases in the USA when in fact evidence was lacking. Did Fauci know about this Seattle situation? If he didn’t, then he is not in the loop at a high enough level to speak clearly to us about what is going on. If he did, then again why would he state declaratively that there were so few cases in America? This does not reflect well on Fauci’s scientific acumen at a time when we need that acumen the most.
The Times article continues:
“What came back confirmed their worst fear. They quickly had a positive test from a local teenager with no recent travel history. The coronavirus had already established itself on American soil without anybody realizing it.
‘It must have been here this entire time,’ Dr. Chu recalled thinking with dread. ‘It’s just everywhere already.’
C.D.C. officials repeatedly said it would not be possible. “If you want to use your test as a screening tool, you would have to check with F.D.A.,” Gayle Langley, an officer at the C.D.C.’s National Center for Immunization and Respiratory Disease, wrote back in an email on Feb. 16. But the F.D.A. could not offer the approval because the lab was not certified as a clinical laboratory under regulations established by the Centers for Medicare & Medicaid Services, a process that could take months.
Dr. Chu and Dr. Lindquist tried repeatedly to wrangle approval to use the Seattle Flu Study. The answers were always no.”
So we have our own example of an acute researcher who saw the potential of disease introduction into the USA (our first case identified on January 21, 2020), saw that flu swabs were available that could immediately shed light on coronavirus cases in America, and was told not to do anything for four weeks until Dr. Chu went ahead and did testing anyway, finding a case of a teenager who had not traveled.
The US death count is currently doubling every three days. Waiting a month to get on with testing involves 10 doubling times. Two to the tenth power is 1024 so anything like a month’s delay exacerbates the problem a thousand-fold. Exponential growth is shocking.
Steven: I had cited Fauci’s downplaying of the U.S. risks at the start of this post.
On rereading footnote [6]
[6] In a March 26 article by Fauci and others, Covid-19 — Navigating the Uncharted, we read:
“If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%.”
I reviewed the NEJM article.
https://www.nejm.org/doi/full/10.1056/NEJMe2002387?query=recirc_curatedRelated_article
This was not a March 26 article, it was a February 28 article posted online then and subsequently included in the March 26 edition of NEJM. I don’t want to be pedantic here, but the difference in dates is 4 weeks, an eternity while exponential growth is running at a doubling time of 2 or 3 days.
“As of February 26, 2020, there had been 14 cases detected in the United States involving travel to China or close contacts with travelers, 3 cases among U.S. citizens repatriated from China, and 42 cases among U.S. passengers repatriated from a cruise ship where the infection had spread.[8] However, given the efficiency of transmission as indicated in the current report, we should be prepared for Covid-19 to gain a foothold throughout the world, including in the United States. Community spread in the United States could require a shift from containment to mitigation strategies such as social distancing in order to reduce transmission. Such strategies could include isolating ill persons (including voluntary isolation at home), school closures, and telecommuting where possible.[9]”
Again, on February 28, 2020, Dr. Fauci fails to mention that very little testing had been done in the USA.
“If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%.”
Additionally, if one understands that in the absence of testing the number of COVID-19 deaths will be underreported, the case fatality rate may be considerably more than 1%.
See
https://www.washingtonpost.com/investigations/coronavirus-death-toll-americans-are-almost-certainly-dying-of-covid-19-but-being-left-out-of-the-official-count/2020/04/05/71d67982-747e-11ea-87da-77a8136c1a6d_story.html
“Coronavirus death toll: Americans are almost certainly dying of covid-19 but being left out of the official count”
I suspect that in the USA we will only figure this out later by tallying the CDC “influenza-like incidences” and associated deaths, and statistically backing out the expected flu counts. The lack of testing leaves far too much room for all of the wild speculation we have seen, by scientists who should know better than to make such declarative statements in the face of so much uncertainty. Testing isn’t even discussed in the February 28 article.
If we can’t test generally in the population to enact epidemiological contact-tracing and other such strategies, we should at least test for presence of COVID-19 in any fatality with any remote possibility or history of influenza-like symptoms before death. Swabs and other appropriate tissue samples should be obtained and kept for later analysis wherever testing is unavaliable at present for cadavers.
Mayo: “If you think Offit is underreacting, I wonder what you think of Ioannidis: https://www.stress.org/stanford-professor-data-indicates-were-severely-overreacting-to-coronavirus
That this is from just a few days ago, linking to his March 17 piece, suggests he still holds this view. He’s right, I think, to worry about consequences, not just economic, but utter social breakdowns–let’s hope not, but prisoners are being released, and it’s not far-fetched for people to need to protect themselves. And what about the extra deaths from operations being put on hold?”
World cases today
“Deaths are a lagging indicator,” said Marc Lipsitch, an epidemiologist at Harvard University, who is modeling the outbreak. Once people are infected, “it takes around three weeks on average for someone to die.”
Not all of the 1 million affected were just recently infected, the disease has been around for a while. On March 26 the global count was 531,000 so we’ve added 500,000 cases in 6 days – in 6 more days we’ll have a count of deaths. Today’s death count is 53,000 and March 26’s count was 24,000. In 6 days the count will be over 100,000, another 6 it will be over 200,000. So if deaths lag by 3 weeks then the death toll associated with today’s million infected cases will be well over 100,000 which is 10% of the million current cases.
I fail to see how the data support Ioannidis’ opinion.
“If we assume that case fatality rate among individuals infected by SARS-CoV-2 is 0.3% in the general population — a mid-range guess from my Diamond Princess analysis — and that 1% of the U.S. population gets infected (about 3.3 million people), this would translate to about 10,000 deaths. This sounds like a huge number, but it is buried within the noise of the estimate of deaths from ‘influenza-like illness.’ If we had not known about a new virus out there, and had not checked individuals with PCR tests, the number of total deaths due to ‘influenza-like illness’ would not seem unusual this year. At most, we might have casually noted that flu this season seems to be a bit worse than average. The media coverage would have been less than for an NBA game between the two most indifferent teams.”
“Some worry that the 68 deaths from Covid-19 in the U.S. as of March 16 will increase exponentially to 680, 6,800, 68,000, 680,000 . . . along with similar catastrophic patterns around the globe. Is that a realistic scenario, or bad science fiction?”
Well here we are at April 2 with 6,100 deaths, we’ll see a death count of over 10,000 in three days. Let’s check back in a few days and see whether my read of statistics garnered from the WHO, Johns Hopkins, the New York Times and other sources is anywhere near Ioannidis’ 0.05% to 1% case fatality ratio. US death counts of 100,000 to 200,000 were discussed today as plausible “if we do everything right”.
https://www.washingtonpost.com/world/2020/03/31/coronavirus-latest-news/
“White House task force projects 100,000 to 240,000 deaths in U.S., even with mitigation efforts”
“Deborah Birx and Anthony S. Fauci, the leaders of the White House task force, emphasized that although the projection of 100,000 to 240,000 deaths were likely, they were hopeful that they could prevent such a high number by adhering to strict mitigation protocols.”
Fauci and Ioannidis are miles apart in their current speculations. The numbers just announced were obtained in part from an epidemiological modeling group at the University of Washington. I’m not sure what’s going on at Stanford.
Given the number of states in the USA still not having any covid lockdown declaration (20 states as of April 2, 2020, Wall Street Journal) the exponential growth will continue. The current death count is doubling every three days and will continue with so much of the country not being serious about doing anything to mitigate this pandemic. If the death rate doubles every 3 days for another 3 weeks, we will be at about 750,000 deaths. This is going to be a very unnerving 3 weeks, and I do not share Ioannidis’ optimism. If the death doubling time miraculously drops to every 6 days right now, we’ll be at 69,000 deaths by April 23. It really doesn’t matter how we slice and dice the case mortality ratio. Even 0.05% of exponential growth is still exponential growth.
Prisoner releases involve non-violent offenders to reduce prison populations, where the virus will spread like wildfire. Overcrowded prisons of rioting prisoners will not work out well. America incarcerates far too many people, and releasing non-violent offenders will work positively in several aspects, justice and disease-wise.
We did not suffer utter social breakdowns during World War 1, the 1918 pandemic, World War II. The history of peoples under challenge is always inspiring – we tend to drop our petty differences to work together for the common good. Good top-down leadership can foster that at this time of great need. If the president could stop calling the governer of Washington state a ‘failed presidential candidate’ and recognize his quick response to a regional problem, better national outcomes will follow. I live in hope.
Mayo: “You’re very critical of the U.S. I’d very much like to know what you would recommend? Are we doing the right thing at this point? Is Canada (which has a much lower incidence)? ”
I would recommend that the president declare a national state of emergency including a national stay at home order; enact wartime powers to compel manufacturers to develop equipment needed; enact quantitative easing (print money) to purchase all said equipment and deploy it to national covid hot spots; shovel out checks to ordinary Americans instead of the wealthiest corporations on the planet so that ordinary Americans can pay their rent and not end up homeless in the middle of a pandemic; compel landlords to halt evictions; and allow any American without health care coverage to join medicare immediately.
Is America doing the right thing at this point? No. 20 state governors still think they and their citizens are somehow immune from this ball of DNA and RNA. Simple physics and chemistry will soon reveal their unfortunate understanding of how the world works. Dealing with a regional catastrophe such as this requires effective leadership from the top, and unfortunately Americans allowed an unprepared citizen to become the president of the whole country. An early act in his administration was to conduct a round of dismissals of officials that the previous administration had put in place after the Ebola crisis (the Ebola crisis blogged at ErrorStatistics in 2014 – worth reviewing again now). When the first case on January 21 2020 was announced in Washington State, the Federal government did not start a top-down all hands on deck test and trace epidemiological strategy. Testing and contact tracing was fumbled for weeks, and when exponential growth is happening, weeks end up being extremely costly. So much talent has been drained from so many important US government agencies, replaced with anyone able to fawn over and compliment the unfortunate choice of leader. Elections have consequences.
Is Canada doing the right thing? Yes, for the most part. Health authorities are provincial agencies, each province runs its own health system, supported also federally. Per capita, far more Canadians have comprhensive health care coverage. When the first cases appeared in British Columbia, testing and tracing began, and a stay-at-home order was quickly issued. My building went into lockdown March 23. The prime minister has worked with the federal government to beef up payments to affected workers. The CBC reports “Prime Minister Justin Trudeau on Wednesday declined to put a specific timeline on how long strict measures could last, saying they would be in place for a number of weeks — and perhaps months.” so we are not being told everything will be hunky-dory by Easter.
Now British Columbia and Washington State are incredibly similar. Very close state/province population counts (7.5 million / 5 million) and Seattle/Vancouver counts (3.5 million / 2.5 million) so we will see what disease trajectories and death counts look like in the months to come. Washington state residents are fortunate to have elected reasonable state leaders, who acted more quickly than most other states have done. But Washington state counts currently (6500 cases, 262 deaths) match the counts of the whole country of Canada (11,000 cases, 131 deaths, Apr 2) more closely than in British Columbia (1,100 cases, 31 deaths). Canada lags the US a bit, so over time we’ll get better comparisons. But top-down leadership is happening more quickly and more effectively in more parts of Canada than America. Sadly in both countries, areas with more right-leaning conservative governing officials have been slower to act and their electors will suffer the consequences. I am currently in British Columbia, not currently under conservative rule, and the Federal government is also not currently conservative. Very fortunate timing and location for me, that I hope many others can experience as soon as possible. British Columbia provincial health officials are acting with remarkable professionalism, and constitute a great source of information and strategy worthy of attention for those who live in areas with poor local and regional leadership.
April 11, 2020 at 12:36 a.m. PDT
The Washington Post
New coronavirus deaths in the United States surpassed 2,000 on Friday, the highest daily tally since the start of the outbreak. The total confirmed dead from the virus in the U.S. is now at 18,586, second only to Italy, and the confirmed worldwide death toll has reached 100,000.
April 17, 2020 11:20 a.m. PDT
Johns Hopkins COVID-19 Dashboard
3.4 million cases worldwide, 149,378 deaths. Thankfully this number is not over 200,000 – global efforts to slow the spread are working where they are being implemented. Curiously, the Johns Hopkins dashboard does not list US total deaths. They list state death counts. So Italy still sits at the top of their death count list, at 22,745 deaths. Looking at the New York Times, the US case count is at 673,000 with 30,809 deaths. Thankfully the spread is slowing in the US, again due to measures implemented in some areas. Future analysis of death counts will eventually yield a more accurate assessment of the toll from this virus, as testing rates and incidence/mortality reporting are currently insufficient.
https://www.washingtonpost.com/investigations/coronavirus-death-toll-americans-are-almost-certainly-dying-of-covid-19-but-being-left-out-of-the-official-count/2020/04/05/71d67982-747e-11ea-87da-77a8136c1a6d_story.html
This won’t be the first under-reported death and case tally in a pandemic.
“A 2013 study [doi: 10.1111/irv.12096] by government and academic researchers suggested that lab-confirmed H1N1 deaths in the United States represented only 1 in 7 fatalities attributable to the disease.”
“To estimate the total fatalities from a disease, scientists often look at ‘excess deaths’ — the number of deaths over and above the average number during a particular period.
The most robust estimates require national statistics that in the United States can take two or three years to compile, according to Cécile Viboud, a National Institutes of Health scientist who co-authored the study estimating the U.S. undercount during the H1N1 flu.”
“In the United States, 2096 laboratory‐confirmed deaths were reported from August 30, 2009–April 6, 2010.[14] Our estimate of 14,800 excess R&C deaths attributable to the pandemic suggests that 1 in ~7 excess deaths were captured by laboratory surveillance. ”
The study concluded:
“In conclusion, we have provided methodological validation for using inpatient mortality databases to monitor the severity of influenza epidemics and proposed broader applications. We hope that this work will inspire the accelerated release of hospitalization and mortality data, so that information on severe outcomes can be released in timelier manner to help guide strategies to mitigate the next emerging infectious disease outbreak.”
Seven years later, inspiration still being hoped for.
https://www.washingtonpost.com/nation/2020/04/24/us-coronavirus-death-toll-surpasses-50000/
April 24, 2020 at 10:07 a.m. PDT
“The coronavirus’s U.S. death toll surged past 50,000 on Friday, marking another grim milestone in the pandemic that has upended life around the globe. Three months after the nation’s first confirmed case, the highly contagious virus has killed at an alarming rate: Just 10 days ago, the number of recorded deaths stood at 25,000.
Experts have warned that the number of reported fatalities likely underestimates the true toll of covid-19, the disease caused by the virus. Amid a national debate over how to count the dead, methods have varied widely from state to state. And the Centers for Disease Control and Prevention initially included only those who tested positive for the virus, even with strict limitations on testing.
The Washington Post has been analyzing data from state health agencies to track every known death in the country. Of the 50,024 fatalities confirmed as of Friday, 21,283 — or about 42 percent — occurred in New York. But while the state has started to see a decrease in its confirmed daily death counts, other parts of the country are beginning to see a surge.”
The social distancing and large gathering bans put in place in late March and early April have indeed slowed the doubling time, with the currently ‘confirmed case’ death count at 50,000. The reported death case count is thankfully no longer doubling every 3 days as I described in my April 3 post – it took 10 days to go from 25,000 to 50,000.
68,000 deaths unfortunately will be the count in a few days – what will Ioannidis conclude? “realistic scenario, or bad science fiction?” Most of the country is nowhere near herd immunity exposure levels, as Ioannidis’ own study in Santa Clara and the recent New York State study show.
As Ioannidis said in his Stat posting of March 17, 2020:
“If we assume that case fatality rate among individuals infected by SARS-CoV-2 is 0.3% in the general population — a mid-range guess from my Diamond Princess analysis — and that 1% of the U.S. population gets infected (about 3.3 million people), this would translate to about 10,000 deaths. This sounds like a huge number, but it is buried within the noise of the estimate of deaths from ‘influenza-like illness.’ If we had not known about a new virus out there, and had not checked individuals with PCR tests, the number of total deaths due to ‘influenza-like illness’ would not seem unusual this year. At most, we might have casually noted that flu this season seems to be a bit worse than average. The media coverage would have been less than for an NBA game between the two most indifferent teams.”
Today, May 4 2020, six weeks later, the Washington Post reports:
68,172 people have died from coronavirus in the U.S.
At least 1,175,000 cases have been reported.
By Joe Fox, Brittany Renee Mayes, Kevin Schaul and Leslie Shapiro
Data as of May. 4 at 10:02 p.m
so with a third of the infection count mentioned by Ioannidis, we see seven times the death count Ioannidis opined we would see.
With many areas ‘opening up’, we head towards the 680,000 of his next paragraph:
“Some worry that the 68 deaths from Covid-19 in the U.S. as of March 16 will increase exponentially to 680, 6,800, 68,000, 680,000 . . . along with similar catastrophic patterns around the globe. Is that a realistic scenario, or bad science fiction?”
How does an epidemiologist not know that this is how exponential growth works in a pandemic? By mid-March, we had already seen what this virus had done in China and Europe.
Mayo: “It’s interesting what you say about likely mode of transmission. What do you think the major route was on the Diamond Princess?”
This virus is amazingly adept at moving around, and time and study will tell how it manages to do this. Partly it appears to be able to begin its viral reproduction in some cases without tripping immune response reactions such as fever, so people remain feeling well. All human speech involves droplet spraying (just watch someone talk on a summer day with the sun setting or rising behind their face) so asymptomatic cases just spray the particles around. How long these droplets can float about remains unknown. They appear to remain viable on certain surfaces, so some surface contact spread may have been involved.
Though the initial decision to try and quarantine in place on the ship appears to have been reasonable given the unknown nature of spread of this new agent, we have subsequently learned that we do not have adequate protocols and procedures to allow such a quarantine to work on a modern cruise ship. The crew quarters are not spacious and a ventilation system that recirculates air across cabins may be part of the problem. I’m not sure that the titans of the cruise ship industry would want to spend the extra money to make cruise ships work better in the all-too-often disease spread scenarios we’ve all heard about. The current covid infections aboard navy vessels rightly requires disembarking personnel as sheltering in place in the cramped quarters of a navy vessel clearly won’t work.
Mayo: “If the major transmission route is respiratory, shouldn’t we be seeing a marked decrease in ordinary flu? I don’t know if we are, the CDC numbers are high.”
I’m unclear on why we would see a decrease in ordinary flu. Those are just other viral particles bopping about this big ball of dirt we live on. Some people are no doubt getting both flu and covid viruses. Sheltering in place will of course also help stem flu spread.
The Seattle study run by Dr. Helen Chu is a flu study, so we may get some data from that study about flu in the midst of the coronavirus pandemic. Some eventual cooperation from the CDC will apparently be required to allow study of both coronavirus and flu virus from the swab samples Dr. Chu collected.
Steven:
thanks for your replies. Here are some more queries.
You wrote:
“This virus is amazingly adept at moving around, and time and study will tell how it manages to do this. …All human speech involves droplet spraying (just watch someone talk on a summer day with the sun setting or rising behind their face) so asymptomatic cases just spray the particles around.”
MAYO: Perhaps you can weigh in on another question I have: how can we test our masks (severely) for effectiveness for this purpose? Everyone’s dreaming up home-made masks now, do those blue disposal surgical(?) masks work (to block the wearer from spreading droplets)? I saw someone spraying different masks to see if whatever was being sprayed gets through, but I’ve no clue what he was spraying.
You wrote:
“The crew quarters are not spacious and a ventilation system that recirculates air across cabins may be part of the problem.”
MAYO: That’s why I find it a little odd that I never hear a hint of this being problematic in buildings, be they dorms or other. I certainly hope it’s not an issue in NYC buildings, but if I was there, I’d change my filters twice as often. I assume it’s not an issue since no one mentions it, and yet, hospitals are careful about this.
You wrote:
“I’m not sure that the titans of the cruise ship industry would want to spend the extra money to make cruise ships work better in the all-too-often disease spread scenarios we’ve all heard about.”
MAYO: In reading about this, it appears the high or higher quality filters, say on planes, is only a bit more expensive. You’d think that if cruise ships are to exist in the future, they’d want to use the higher quality and advertise that they do so. I also read that Chen, the researcher I cite in my post, is developing a ventilation system for ships that prevents viral spreading. I might write to him.
You wrote:
“I’m unclear on why we would see a decrease in ordinary flu. Those are just other viral particles bopping about this big ball of dirt we live on. Some people are no doubt getting both flu and covid viruses. Sheltering in place will of course also help stem flu spread.”
MAYO:Are you being consistent? That was my point, that it seems we should be seeing a decrease in cases of ordinary flu (given the sheltering and distancing), and if we’re not, what then? CDC gives a weekly estimate.
From https://www.cdc.gov/flu/weekly/index.htm
“Weekly U.S. Influenza Surveillance Report
Key Updates for Week 13, ending March 28, 2020
Note: The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.
Laboratory confirmed flu activity as reported by clinical laboratories continues to decrease sharply and is now low. Influenza-like illness activity, while lower than last week, is still elevated. Influenza severity indicators remain moderate to low overall, but hospitalization rates differ by age group, with high rates among children and young adults.
Illness
Outpatient Illness: ILINet
Visits to health care providers for influenza-like illness (ILI) decreased from 6.3% last week to 5.4% this week. All regions are above their baselines.
Based on National Center for Health Statistics (NCHS) mortality surveillance data available on March 26, 2020, 8.2% of the deaths occurring during the week ending March 21, 2020 (week 12) were due to P&I. This percentage is above the epidemic threshold of 7.2% for week 12.”
Flu data indicators do not seem to be showing any marked drop. However with the coronavirus activity in the mix, as they note, data need to be interpreted with caution.
Much of the nation not being under lockdown, the flu seems to be at its usual levels as indicated by pneumonia and influenza-like illness. Laboratory confirmed flu activity always declines at this time of year, that seems also to be happening as expected.
MAYO: “Perhaps you can weigh in on another question I have: how can we test our masks (severely) for effectiveness for this purpose? Everyone’s dreaming up home-made masks now, do those blue disposal surgical(?) masks work (to block the wearer from spreading droplets)? I saw someone spraying different masks to see if whatever was being sprayed gets through, but I’ve no clue what he was spraying.”
Testing a mask is not trivial. Viral particles are tiny. A truly severe test would involve wearing a mask in a lab, talking away for a few minutes with a little air-sampling gizmo, then swabbing the surfaces around the mask-wearer and testing all of that for viral bits with qPCR or other genetic particle detection assays.
Just about any piece of cloth put over the face will catch some droplets, but not all. There’s plenty of leakage around the edges of the mask as you breathe out.
I think the main value of masks is to give the wearer some sense of doing something to protect against an invisible foe. But a false sense of security can lull people into unsafe behaviour as well, so there is as yet no clear answer as to the benefit of wearing a bandana, a scarf or a surgical mask.
The eyes are another route in for the virus, so a mask without an eye shield is no defense against this virus.
The burka may yet become the fashion choice of the year.
MAYO: “You wrote:
‘The crew quarters are not spacious and a ventilation system that recirculates air across cabins may be part of the problem.’
That’s why I find it a little odd that I never hear a hint of this being problematic in buildings, be they dorms or other. I certainly hope it’s not an issue in NYC buildings, but if I was there, I’d change my filters twice as often. I assume it’s not an issue since no one mentions it, and yet, hospitals are careful about this.”
Yes, hospitals are careful about this. Measles virus particles can remain airborne (actually stick to dust particles) and viable for a couple of hours, so hospitals have to deal with that. Airplanes have better filtration systems than cruise ships (able to capture smaller particles), perhaps that will change in cruise ships. Measles particles in dorm or other building air isn’t such a big problem anymore, as the vast majority of the dorm occupants have had the measles or had a vaccine.
From a meta-analysis of several studies (DOI: 10.1111/j.1600-0668.2006.00445.x)
Click to access li-et-al.-ventilation-1.pdf
“There is strong and sufficient evidence to demonstrate the association between ventilation, air movements in buildings and the transmission/spread of infectious diseases such as measles, tuberculosis, chickenpox, influenza, smallpox and SARS. There is insufficient data to specify and quantify the minimum ventilation requirements in hospitals, schools, offices, homes and isolation rooms in relation to spread of infectious diseases via the airborne route.”
This came out April 6 by philosopher Peter Singer and Michael Plant: “When Will the Pandemic Cure Be Worse Than the Disease?”
It uses data from the Diamond Princess.
https://www.project-syndicate.org/commentary/when-will-lockdowns-be-worse-than-covid19-by-peter-singer-and-michael-plant-2020-04
The hunger games are on.
Why do we bother with any health care efforts at all? The economic benefits of saving human lives just never add up. When Bob is having a heart attack at the office building, why invade that building with a bunch of EMTs? They disrupt the business, distract the other employees from their tasks, and eat in to shareholder profits. The resultant loss of government services puts many others in peril.
Better to leave Bob to recover, and get back to work.
Exponential growth is a phenomenon not well understood by many people. Nuclear physicists understood it all too well as they developed the A-bombs of World War II. Biologists and doctors who deal with cancer understand the end effect of cellular exponential growth all too well. As a biostatistician I face the resultant survival data on a regular basis.
Paul Frijters clearly doesn’t understand exponential growth, opining on March 21st that “The worldwide death toll of corona is even now no higher than a thousand per day”. Today, on April 9, the daily death toll was 7,000 and next week we will see death tolls of 14,000 per day while country leaders reject a global response and even responses within their own nations. What is Paul Frijter’s upper limit on daily excess deaths, which are preventable when people around the planet cooperate with one another, as seen previously for SARS, MERS and Ebola? Does he even have an upper limit? Is any level of daily death just fine, so long as we avoid interfering with stock market fundamentals?
“Second, making trade-offs requires converting different outcomes into a single unit of value. A problem with the current conversations about whether we should strangle the economy to save lives is that we cannot directly compare ‘lives saved’ against ‘lost GDP.’ We need to put them into some common unit.” say Singer and Plant.
Another mathematical phenomenon not widely appreciated is that in order to declare one thing “better” or “worse” than another, one must reduce to one dimension to rank things as “better” or “worse”. You just can’t do it in two or more dimensions. Anyone knows 2 is bigger than 1, and when it’s 2 donuts versus one donut, well 2 donuts is clearly better than one donut. But in two dimensions, is (3, 2) better than (4, 1)? Or is (5, 4) better than (4, 9)? Hence Singer and Plant discuss the need to find a common unit – one that clearly shows that 200 million people should die so that an outcome of “greater” value can be clearly logged in the ledgers of mankind. “Two hundred million people proudly lined up to die, so that the Dow Jones Industrial Average decline could be minimized. We salute those brave souls, who understood that altering the trajectory of our largest industries was just an unimaginable ask. The profits of giant pharmaceutical companies was certainly more important than the lives of unnecessary and inconvenient unwashed masses.”
The messy thing about life is that it is more than one dimensional. So we all struggle to work our way through multiple dimensions, charting a course to a place in those multiple dimensions that seems that it might yield a less than terrifying daily existence.
Most people recoil from a game plan that involves doing nothing, and devil take the hindmost. Many animal species do not have the luxury of understanding the myriad complexities we face on a daily basis – an approaching hurricane, a pride of lions near by, an exponentially increasing infectious microbe. Should we really have told Jenner to go away with his cowpox crazy idea? Do we all now decry all medical treatment, and banish the medical professionals? Why bother with the soap industry and all that wasted time washing hands? Tea leaves and goat entrails really told us all we ever needed to know. 2000 years of cultural and scientific development were all for naught in the end.
“It pains us to say it, but US President Donald Trump is right: ‘We cannot let the cure be worse than the disease.’ ”
Donald Trump has a litany of tens of thousands of lies, documented and debunked by a myriad of hard working journalists and others. It should pain you to say that he is right. He has been proven wrong repeatedly. Strong action to start testing, quarantining and contact tracing in January 2020 when our first cases were uncovered would have involved some hardship for a few tens of thousands of people for a few months. Ignoring the issue as a pathogen spread exponentially was a choice. I and many others reject such a choice. The initial cure was not undertaken when it had a far better chance of succeeding. Donald Trump is decidedly not right.
John Ioannidis and others opine that disaster never struck us when SARS came on the scene, nor for MERS, nor Ebola. Why all the fuss? Disaster after disaster predicted in the past never came to be. They fail to review the extraordinary steps taken to avert a pandemic then. With all of these recent episodes, testing, contact tracing and quarantining done aggressively and early kept the disease down in numbers and Wall Street was left to induce a financial disaster with derivative instruments and liar loans rather than be taken down by a microbial pathogen. In the Ebola crisis, decent foreign relations implemented in the last United States presidential administration allowed the USA to send thousands of troops and medical staff to Africa to deal with the crisis at its origin. Now, with relations with China strained by petty tweets and insults and ridiculous trading strategies, no response at the initial epicenter was undertaken. Once the problem hit our shores, still nothing. The very government response teams, trained to handle just this problem, dismissed months and years ago because a business man of many bankrupted businesses, elected as president, thought people sitting around doing nothing was just a dumb idea. Those people weren’t doing nothing, they were preparing for just this crisis.
What people need on a regular basis is a roof over their head and daily food and clean water, not a ‘livelihood’ at a medical insurance company, telling people that their health care needs are not covered, or at an oil extraction company, telling people that their only option for mobility is to use a machine that emits gasses harmful to their very existence.
We have plenty of resources, all we lack is the will to take the necessary societal actions to buckle down and ensure that everyone can shelter somewhere without being evicted, and have some level of access to basic amounts of food and water. That sheltering could have been borne by a much smaller number of people earlier on. But because a poorly prepared leader made bad choice after choice, Frijters, Singer and Plant are happy to see millions die so that ‘livelihoods’ are not impacted. The livelihoods of the families of today’s 7,000 dead seem not to matter.
I may be wrong about all this, society may be changing and I just don’t see it, with a steady stock market readout as the only dimension worthy of consideration in all decisions of life and death. But that’s not what I see around me. I see all kinds of people buckling down to deal with this disease, willingly choosing to use less, do with less, survive with less, and divert resources to dodge a microbe and keep more of us alive, albeit with less toilet paper, than just casting 200 million people to the microbial wolves. I reject the morbid calculations of Frijters, and join with my community to share in the burden of working to ensure that as many of us as possible make it through this microbial disaster.
Steven: I’ve always rejected those utilitarian measures of the value of a year of life and such. Singer was vilified some years ago for his stance on infanticide.
While Frijters, Singer and Plant wring their hands about the economy, plenty of people are taking real action to help their fellow citizens weather this pandemic, creating economic flows appropriate to supporting others in the effort to save all lives.
A truck stop operator in Nova Scotia, Canada figures out some economic activity appropriate for truckers delivering the goods we all rely on:
https://www.cbc.ca/news/canada/nova-scotia/free-hot-meals-for-truck-drivers-nova-scotia-1.5514211
Air and water pollution is down:
https://www.telegraph.co.uk/travel/news/coronavirus-nature-environment-swans-venice-clear-skies-china/
Air pollution is of course a major problem when a respiratory pandemic unfolds.
Though fossil fuel corporations will go bankrupt due to excessive junk bond financing, renewable power companies continue to expand:
We will reconstruct a new global economy in the aftermath of this pandemic, and that economy will be better tuned to how we need to live going forward. If we are capable of learning anything, and have the international willpower to cooperate instead of compete excessively, much economic good will result from this unfortunate pandemic.
A global massive effort to integrate data from various sources is under way. Turning it into information quality is challenging, the initial focus is on standardization of terms https://www.medrxiv.org/content/10.1101/2020.04.02.20051284v1
This is unusual in that it combines self reporting via smartphone apps with “official” statistics. It provides some triangulation capabilities and an opportunity for severe testing of models and exit strategies.
Data from the diamond Princess continues to figure even in today’s modeling of prevalence:https://science.sciencemag.org/content/early/2020/05/12/science.abc3517
But it would be better to get reliable serological data, than just fit models.
Pingback: The Corona Princess: Learning from a petri dish cruise (i) – a. → all Story at a.
It’s July 31, 2020. An article to come out yesterday employs the Diamond Princess to argue for aerosol transmission–finally–but there’s something that seems off in the study. I’m absolutely not a specialist. I’m going to ask Chen what he thinks.
It’s intriguing to read the comments from back in March. In May and June I was so busy with my LSE Graduate PH500 Seminar on controversies in Phil Stat, that I didn’t keep up as much. I’m glad I have the record.
Aug 1, 2020: This Norweigan cruise ship had 4 sick crew “several days ago”, but they claim their symptoms were not indicative of covid-19. They were not tested for covid until yesterday–all 4 had it. Now 36 crew, in total, have tested positive. In the mean time, all the passengers have left the ship. They said they read about the outbreak in the papers, before being called and advised to isolate.
https://www.maritime-executive.com/article/hurtigruten-crew-members-test-positive-for-covid-19-on-a-norway-cruise
https://www.france24.com/en/20200801-36-crew-test-positive-for-virus-on-norwegian-cruise-ship
I’m curious what these symptoms were that they dismissed as “couldn’t be covid”, since there are so many beyond the most common. they don’t say. There were 2 one-week trips with this same crew in July. I will follow the story here and on twitter.
A cruise ship called the Gaugin now has a suspected covid case. It only returned to see a couple of weeks ago. It sounds like a great cruise. https://www.maritime-executive.com/article/one-suspected-covid-19-case-on-cruise-ship-paul-gauguin
Amundsen now has 64 infected among crew and passengers. However, since the passengers have long since embarked, they might not find out about all of them. https://www.maritime-executive.com/article/covid-19-cases-rise-on-one-cruise-ship-while-others-test-negative
Aug 24 https://wwwnc.cdc.gov/eid/article/26/11/20-1165-t2
The Washington Post has an article today reviewing Ioannidis’ long list of saying stuff about the pandemic.
https://www.washingtonpost.com/dc-md-va/2020/12/16/john-ioannidis-coronavirus-lockdowns-fox-news/
including this bit about a video he posted on YouTube: “The video would be viewed more than a half-million times on YouTube before it disappeared. Six weeks after it was uploaded, the footage of Ioannidis was removed by YouTube, which said the interview with one of the world’s foremost epidemiologists had violated its policies on covid-19 misinformation.”
and this tweet from the University of North Carolina’s researcher Alex Rubinsteyn concerning Ioannidis’ bizarre medRxiv paper that spectacularly misestimated the COVID-19 infection fatality rate via a cobbled study of cases recruited via facebook:
“What a weird turn to see John Ioannidis pushing one of sloppiest studies in the deluge of Covid-19 papers. If he weren’t an author I would expect the Stanford serostudy to show up in one of his talks as a particularly potent cocktail of bad research practices.”